Reproduced from: Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. London: RCP; 2017.
نبذة عملية
الفكرة السريرية الشاملة
يُعد مقياس الإنذار المبكر الوطني 2 (National Early Warning Score 2 – NEWS2) حجر الأساس السريري الموحد لتقييم حدة التدهور الفسيولوجي واصطياد الإشارات المبكرة للانهيار قبل السريري للمرضى البالغين في الأجنحة. تم ابتكاره واعتماده من الكلية الملكية للأطباء بمقاطعة لندن كبروتوكول معياري يعزز سرعة التدخل، ويحدد بوصلة الطبيب المناوب لاتخاذ قرار الإحالة العاجل نحو وحدات العناية المركزة (ICU).
قراءة المناوب العملية: NEWS2 ليس رقماً للتوثيق فقط. هو لغة مشتركة بين التمريض، طبيب الجناح، المناوب، فريق الاستجابة السريعة، والعناية المركزة. قيمته الحقيقية أنه يمنع أن يبقى التدهور موزعاً بين أرقام تبدو منفصلة: تنفس أسرع، ضغط أقل، نبض أعلى، وعي متغير، أو حاجة جديدة للأكسجين. عندما تجمعها في NEWS2، يتحول الانطباع إلى إنذار قابل للتصرف.
قاعدة عملية للمناوب: لا تتعامل مع NEWS2 كآلة قرار عمياء. الدرجة العالية تفرض التصعيد، لكن الدرجة المنخفضة لا تلغي القلق السريري إذا كان مسار المريض يتدهور. الرقم يساعدك أن ترى الخطر، لكنه لا يعفيك من قراءة القصة، الفحص، سرعة التدهور، والاستجابة للعلاج الأولي.
متى يكون NEWS2 مفيداً جداً؟
في الأجنحة: عندما يكون المريض “ليس على ما يرام” لكن الصورة غير مكتملة بعد.
في المناوبة الليلية: عندما تحتاج لغة رقمية واضحة لتبرير التصعيد أو طلب الحضور.
عند تسليم المناوبة: لأن تغير NEWS2 عبر الزمن أهم من رقم منفرد معزول.
عند الاشتباه بالإنتان أو الفشل التنفسي أو الصدمة: لأنه يلتقط الانحرافات الفسيولوجية قبل اكتمال الانهيار.
عند قرار العناية المركزة: لأنه يضع المريض في مستوى خطورة واضح، لكنه يجب أن يُدمج مع التقييم السريري والغازات والتحاليل ومسار المرض.
فحوص واستقصاءات
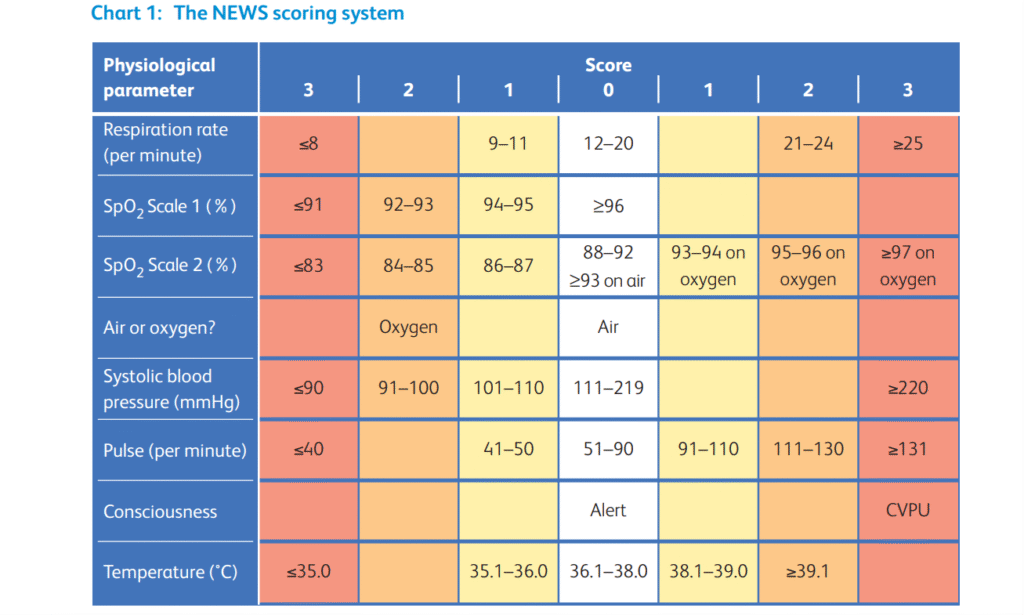
جدول المتغيرات الفيزيولوجية: حاسبة الدرجات
ملاحظة للمناوب:مرّر الجدول يميناً ويساراً على الموبايل لمشاهدة كافة الدرجات. احسب الدرجة من أسوأ قيمة حديثة موثوقة، ثم اسأل دائماً: هل الرقم ثابت؟ أم في صعود؟
المؤشر الحيوي
مخاطر (3)
مخاطر (2)
مخاطر (1)
طبيعي (0)
مخاطر (1)
مخاطر (2)
مخاطر (3)
معدل التنفس
≤ 8
9 – 11
12 – 20
21 – 24
≥ 25
إشباع الأكسجين (Scale 1)
≤ 91
92 – 93
94 – 95
≥ 96
الأكسجين الداعم
نعم (موصول)
هواء الغرفة
ضغط الدم الانقباضي
≤ 90
91 – 100
101 – 110
111 – 219
≥ 220
النبض / دقيقة
≤ 40
41 – 50
51 – 90
91 – 110
111 – 130
≥ 131
مستوى الوعي
أو تشوش حديث (V, P, U)
واعي ومتنبه (Alert)
الحرارة (°C)
≤ 35.0
35.1 – 36.0
36.1 – 38.0
38.1 – 39.0
≥ 39.1
ملاحظات حسابية مهمة للمناوب
الأكسجين الداعم: وجود أي أكسجين موصول للمريض يضيف درجتين في NEWS2، حتى لو كان الإشباع يبدو مقبولاً.
الوعي: أي تشوش حديث أو استجابة لـ Voice/Pain/Unresponsive تُحسب كاختلال وعي خطير، ولا تُفسر تلقائياً كنعاس أو تعب.
درجة 3 في متغير واحد: حتى لو كان المجموع الكلي منخفضاً نسبياً، وجود “Red Score” في مؤشر واحد يجب أن يرفع مستوى القلق ويتطلب مراجعة سريرية عاجلة.
Scale 1 وScale 2: الجدول أعلاه يعرض Scale 1. عند مرضى COPD أو المعرضين لفرط ثاني أكسيد الكربون، يجب استخدام Scale 2 فقط إذا كان موثقاً طبياً ومقرراً محلياً، ولا يجوز إنقاص الأكسجين أو قبول إشباع منخفض دون سبب واضح وخطة غازات.
الاتجاه أهم من الرقم: NEWS2 4 يصعد بسرعة قد يكون أخطر من NEWS2 5 ثابت عند مريض مزمن. راقب المسار لا الرقم فقط.
خوارزمية التصعيد
خوارزمية الاستجابة السريرية حسب الدرجة
يتم جمع النقاط للحصول على الرقم الإجمالي. توصي البروتوكولات المرجعية بما يلي:
الدرجة 0 – 4 (خطورة منخفضة): مراقبة وتمريض روتيني، مع تقييم الفايتالز كل 4 إلى 6 ساعات. ملاحظة: إذا تضمنت الدرجة 3 نقاط لمتغير وحيد، تتطلب مراجعة من قبل طبيب الجناح.
الدرجة 5 – 6 (خطورة متوسطة): نداء للرعاية. تتطلب تقييماً مباشراً من قبل الطبيب المناوب المؤهل ضمن حد أقصاه 60 دقيقة. احتمالية التدهور السريري قائمة.
الدرجة ≥ 7 (خطورة عالية جداً): استنفار طارئ. تتطلب مراجعة فورية وتدقيقاً من فريق العناية المشددة (Critical Care Outreach Team)، وغالباً يتطلب الأمر نقل المريض لوحدة العناية الفائقة أو المراقبة الحثيثة العالية (HDU).
طريقة التفكير العملي عند كل درجة
NEWS2 0: لا يعني أن المريض “مضمون”، بل يعني أن الفسيولوجيا الحالية مستقرة. استمر بالمراقبة حسب السياق المرضي.
NEWS2 1 – 4: اسأل: هل هناك درجة 3 منفردة؟ هل الدرجة في صعود؟ هل المريض تغير سريرياً؟ إذا نعم، لا تنتظر أن يصبح المجموع 5.
NEWS2 5 – 6: هذه ليست “درجة متوسطة مريحة”. هي عتبة مراجعة عاجلة. يجب تقييم السبب، بدء العلاج الأولي، وتحديد هل يحتاج المريض تصعيداً أو مراقبة أو غازات أو تصويراً أو سوائل أو مضاداً حيوياً أو مراجعة عناية.
NEWS2 ≥ 7: تعامل معها كإنذار انهيار قريب. اذهب للمريض، قيّم ABCDE، استدعِ الدعم المناسب، ولا تكتفِ بتوثيق الرقم في الملف.
خوارزمية ABCDE للمناوب عند NEWS2 مرتفع
A – Airway: هل الطريق الهوائي سالك؟ هل يوجد صرير، قيء، وذمة، نزف، نقص وعي، أو خطر استنشاق؟
B – Breathing: معدل التنفس، SpO₂، الحاجة للأكسجين، الجهد التنفسي، أصوات الرئة، غازات الدم، واحتمال فشل تنفسي.
C – Circulation: الضغط، النبض، الإرواء المحيطي، الإدرار، النزف، علامات الصدمة، الحاجة لسوائل أو رافعات ضغط.
D – Disability: الوعي، التشوش الحديث، GCS، السكر، الاختلاجات، الأدوية المثبطة للوعي.
خلاصة مناوبة: NEWS2 لا يطلب منك أن “تحسب ثم تنتظر”. هو يطلب منك أن “تحسب ثم تتصرف”. الرقم هو بداية التقييم وليس نهايته.
مؤشرات الخطورة
متى يجب الاتصال وتشريك العناية المركزة؟
إن النقل إلى العناية لا يعتمد حصرياً على الأرقام، بل على التقييم الإكلينيكي الشامل والتوجه السريري الدؤوب:
NEWS2 ≥ 7 المُطلق: مؤشر قسري ومستقل يفترض حاجة المريض لبيئة الإنعاش. الدراسات تؤكد أن التأخر في الاستجابة لدرجة 7 يزيد من معدلات الوفيات بشكل هائل.
الانهيار السريع (Rapid Trajectory): حتى وإن كان المقياس الأساسي منخفضاً; الصعود الصاروخي بمقدار (+2 نقاط) أو أكثر خلال نافذة زمنية ضيقة جداً يعكس تدهوراً انسيابياً حاداً يسبق التوقف القلبي التنفسي.
حالة الـ (NEWS2 ≥ 5) المعندة: الدرجات المتوسطة التي تأبى الاستجابة للمداخلات الإسعافية الأولية كالسوائل الوريدية أو الأكسجين.
الرايات الحمراء المطلقة التي تتجاوز السكور
الانهيار التنفسي (Respiratory Failure): تدهور الغازات الشريانية المحتم، استنفاذ العضلات التنفسية المساعدة، والحاجة لدعم تنفسي آلي أو غير الغازي (BiPAP/CPAP).
الانهيار الهيموديناميكي (Hemodynamic Shock): صدمة جهازية لا تستجيب لصدمات السوائل الكبيرة (Fluid Bolus)، وتتطلب تسريب رافعات الضغط الوريدية (Vasopressors).
الانهيار العصبي (Neurological Deficit): انحدار مفاجئ في مقياس غلاسكو (GCS ≤ 8)، أو اختلاجات معندة متكررة (Status Epilepticus).
الكوارث الاستقلابية: حماض استقلابي عنيف مهدد للحياة، اضطراب شوارد صاعق (Hyperkalemia)، أو الحاجة الملحة لغسيل كلوي طارئ.
مؤشرات إضافية لا تنتظر الرقم
زيادة الحاجة للأكسجين: مريض كان على هواء الغرفة ثم احتاج أوكسجيناً متصاعداً، حتى لو لم يصل NEWS2 إلى 7 بعد.
تدهور الوعي الحديث: التشوش الجديد علامة فشل جهازي أو عصبي حتى يثبت العكس.
انخفاض الضغط مع علامات سوء إرواء: برودة أطراف، تأخر امتلاء شعري، قلة إدرار، لاكتات مرتفع.
تسرع تنفس شديد: معدل التنفس غالباً أول علامة تدهور، ولا يجوز تجاهله لأنه “المريض قلق”.
عدم الاستجابة للعلاج الأولي: استمرار نقص الأكسجة، الضغط المنخفض، أو التشوش بعد التدخلات الأولى يستدعي تصعيداً مبكراً.
خطة التدبير
ماذا يفعل المناوب عملياً عند NEWS2 ≥ 5؟
اذهب للمريض: لا تعالج الرقم من الهاتف فقط. افحص ABCDE بنفسك أو مع الفريق.
أكد القياسات: أعد قياس العلامات الحيوية إذا كانت غير منطقية، لكن لا تستخدم إعادة القياس كوسيلة لتأخير التصعيد.
ابحث عن السبب: إنتان، نزف، فشل تنفسي، احتشاء، صمة رئوية، تجفاف، اضطراب نظم، تأثير دوائي، اختلاط جراحي، أو تدهور عصبي.
ابدأ التدخل الأولي: أكسجين مناسب، قثطرة وريدية، سوائل عند الصدمة المناسبة، تحاليل عاجلة، غازات، لاكتات، سكر، ECG، زراعة وصادات عند الاشتباه بالإنتان، وتصوير حسب الحالة.
حدد مستوى الرعاية: جناح مع مراقبة متقاربة، HDU، أو ICU.
اتصل بوضوح: عند التصعيد استخدم SBAR: الدرجة، سبب القلق، مسار التدهور، ما فعلته، وما تحتاجه الآن.
متى يكون طلب العناية المشددة مقنعاً؟
NEWS2 ≥ 7 مع تدهور سريري أو حاجة أكسجين أو صدمة أو اختلال وعي.
NEWS2 ≥ 5 لا يتحسن بعد التدخل الأولي.
ارتفاع سريع في الدرجة خلال ساعات قليلة.
حاجة محتملة لـ NIV، CPAP/BiPAP، تنبيب، مراقبة غازية، رافعات ضغط، أو غسيل كلوي إسعافي.
وجود مرض أساسي خطير مع احتياطي فيزيولوجي قليل، مثل COPD شديد، قصور قلب متقدم، تثبيط مناعة، أو ما بعد عمل جراحي كبير.
قلق سريري قوي رغم رقم غير مرتفع: الطبيب يرى شيئاً لا تلتقطه الدرجة بعد.
صيغة اتصال جاهزة للعناية أو فريق الاستجابة
“معك د. (…) من جناح (…). أتصل بخصوص مريض عمره (…) لديه NEWS2 الآن (…) بعد أن كان (…). سبب القلق الأساسي هو (…): تنفس/ضغط/وعي/أكسجين. قمت بـ (…). المريض لم يتحسن/يتدهور بسرعة. أحتاج تقييم عناية/استجابة عاجلة الآن، وأعتقد أنه قد يحتاج إلى (…).”
نقطة إنقاذ عملية: لا تقل فقط “NEWS2 سبعة”. قل لماذا سبعة، وكيف وصل إلى سبعة، وما الذي فشل في التحسن، وما التدخل الذي تتوقع أن يحتاجه.
نقاط وفخاخ
فخاخ المناوبة المتكررة
فخ الرقم المنخفض: مريض يتدهور بسرعة قد يكون خطراً قبل أن يصل NEWS2 إلى 7.
فخ الأكسجين الذي يخفي الخطر: الإشباع المقبول على أكسجين عالٍ ليس طبيعياً. الحاجة للأكسجين نفسها علامة خطر.
فخ التنفس المهمل: معدل التنفس من أكثر المؤشرات حساسية للتدهور، لكنه أكثر مؤشر يتم تجاهله أو تقديره بشكل غير دقيق.
فخ التشوش: التشوش الحديث ليس “نعاساً” حتى يثبت العكس. فكر بنقص أكسجة، إنتان، صدمة، اضطراب سكر، أدوية، أو سبب عصبي.
فخ انتظار التحاليل: لا تنتظر اللاكتات أو الغازات إذا كان المريض منهاراً سريرياً.
فخ السكور بدل الفحص: NEWS2 لا يفحص البطن، لا يسمع الرئة، لا يرى النزف، ولا يقرأ حدسك السريري. افحص المريض.
فخ التصعيد المتأخر: الاتصال بالعناية بعد فشل كل شيء أسوأ من الاتصال المبكر عند بداية الانهيار.
لآلئ عملية للمناوب
إذا صعد NEWS2، ابحث عن السبب لا عن الرقم فقط.
إذا كان NEWS2 ≥ 5، فكر: هل أحتاج مراجعة خلال ساعة؟ هل أحتاج غازات؟ هل أحتاج فريق أعلى؟
إذا كان NEWS2 ≥ 7، فكر: هل يحتاج المريض مراقبة مستمرة أو HDU/ICU؟
إذا كانت درجة واحدة = 3، لا تطمئن إلى المجموع المنخفض.
إذا تغير الوعي أو زادت الحاجة للأكسجين، صعّد مبكراً.
إذا عالجت السبب وتحسن NEWS2، وثّق الاستجابة وخطة المراقبة القادمة.
خلاصة مناوبة سريعة
NEWS2 0 – 4: خطورة منخفضة، لكن انتبه لدرجة 3 منفردة أو صعود سريع.
On-Call Note: NEWS2 Scoring Criteria and ICU Escalation Directives
Reproduced from: Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. London: RCP; 2017.
Clinical Overview
The clinical purpose of NEWS2
The National Early Warning Score 2 (NEWS2) is a standardized bedside scoring system designed to detect acute physiological deterioration in adult inpatients. It was developed and endorsed by the Royal College of Physicians to support earlier recognition of clinical decline, trigger timely escalation, and guide the on-call clinician toward appropriate senior review, high-dependency monitoring, or ICU-level care when needed.
Practical on-call reading: NEWS2 is not just a number to document in the chart. It is a shared language between nursing staff, ward doctors, on-call clinicians, rapid response teams, and critical care. Its real value is that it prevents deterioration from being scattered across separate observations: a faster respiratory rate, lower blood pressure, rising pulse, new confusion, or new oxygen requirement. When these signals are aggregated into NEWS2, clinical concern becomes an actionable warning.
Practical on-call rule: Do not treat NEWS2 as a blind decision machine. A high score mandates escalation, but a low score does not cancel clinical concern if the patient is deteriorating. The score helps you see risk, but it does not replace history, examination, trajectory, response to treatment, and bedside judgement.
When NEWS2 is especially useful
On the ward: When the patient is “not quite right” and the clinical picture is still incomplete.
During night shifts: When a numerical language is needed to justify escalation, attendance, or senior review.
During handover: Because the trend in NEWS2 over time is often more important than a single isolated value.
In suspected sepsis, respiratory failure, or shock: NEWS2 can capture physiological drift before full collapse is obvious.
When considering critical care: NEWS2 places the patient into a structured risk band, but it must be integrated with clinical assessment, blood gases, laboratory results, comorbidities, and disease trajectory.
Investigations and Monitoring
Physiological parameter triage: NEWS2 calculator
Mobile navigation note:Swipe the table horizontally to view all score metrics. Calculate the score from the most recent reliable worst value, then always ask: is this score stable, or is it rising?
Physiological Parameter
Score (3)
Score (2)
Score (1)
Normal (0)
Score (1)
Score (2)
Score (3)
Respiration Rate
≤ 8
9 - 11
12 - 20
21 - 24
≥ 25
Oxygen Saturation (Scale 1)
≤ 91
92 - 93
94 - 95
≥ 96
Air or Oxygen?
Oxygen
Air
Systolic BP
≤ 90
91 - 100
101 - 110
111 - 219
≥ 220
Pulse
≤ 40
41 - 50
51 - 90
91 - 110
111 - 130
≥ 131
Consciousness
New confusion or CVPU
Alert
Temperature (°C)
≤ 35.0
35.1 - 36.0
36.1 - 38.0
38.1 - 39.0
≥ 39.1
Important scoring notes for the on-call clinician
Supplemental oxygen: Any oxygen being delivered to the patient adds 2 points in NEWS2, even if the saturation looks acceptable.
Consciousness: New confusion or response only to Voice, Pain, or Unresponsive is a serious consciousness abnormality and should not be dismissed as simple tiredness.
Single parameter score of 3: Even if the aggregate score is not high, a red score in one physiological parameter should raise concern and trigger urgent clinical review.
Scale 1 and Scale 2: The table above shows Scale 1. In patients with COPD or risk of hypercapnic respiratory failure, Scale 2 should only be used if clinically documented and locally agreed. Do not reduce oxygen or accept low saturations without a clear reason and a blood-gas plan.
Trend matters more than a single number: NEWS2 4 that is rising quickly may be more dangerous than NEWS2 5 that is stable in a chronic patient. Follow the trajectory, not the number alone.
Escalation Algorithm
Clinical response by aggregate score
NEWS2 points are systematically aggregated to define the urgency of clinical response. Reference protocols recommend the following escalation logic:
Score 0-4: Low-risk profile. Standard ward observation and routine nursing monitoring, with vital-sign reassessment typically every 4 to 6 hours according to local policy. Exception: any single parameter scoring 3 explicitly requires urgent registered clinician review.
Score 5-6: Medium-risk profile. This triggers a formal response alert. It requires direct hands-on clinical evaluation by a qualified clinician, usually within a maximum 60-minute window. The probability of clinical deterioration is significant.
Score ≥ 7: High-risk emergency. This activates emergency escalation. It requires immediate review by a team with critical-care competencies, such as a Critical Care Outreach Team, and often consideration of transfer to HDU or ICU-level care.
Practical interpretation at each score level
NEWS2 0: This does not mean the patient is guaranteed safe. It means current physiology is stable. Continue monitoring according to the illness context.
NEWS2 1-4: Ask: is there a single parameter scoring 3? Is the score rising? Has the patient changed clinically? If yes, do not wait for the aggregate score to reach 5.
NEWS2 5-6: This is not a comfortable “moderate” score. It is an urgent review threshold. Find the cause, start initial treatment, and decide whether the patient needs escalation, monitoring, blood gases, imaging, fluids, antibiotics, or critical-care review.
NEWS2 ≥ 7: Treat this as a near-collapse warning. Go to the patient, assess ABCDE, call appropriate support, and do not simply document the number in the chart.
ABCDE algorithm for elevated NEWS2
A - Airway: Is the airway patent? Is there stridor, vomiting, edema, bleeding, reduced consciousness, or aspiration risk?
B - Breathing: Respiratory rate, SpO₂, oxygen requirement, work of breathing, lung sounds, blood gases, and risk of respiratory failure.
C - Circulation: Blood pressure, pulse, peripheral perfusion, urine output, bleeding, shock signs, and need for fluids or vasopressors.
D - Disability: Consciousness, new confusion, GCS, glucose, seizures, sedative medications, and neurological deterioration.
E - Exposure: Temperature, rash, sepsis signs, pain, hidden bleeding, lines, drains, wounds, and the likely source of deterioration.
Rapid on-call summary: NEWS2 does not ask you to calculate and wait. It asks you to calculate and act. The score is the beginning of assessment, not the end.
Red Flags
When to call or involve critical care
ICU or HDU escalation does not depend on numbers alone. It depends on the aggregate NEWS2 score, the clinical trajectory, the response to initial treatment, and the patient’s physiological reserve.
Absolute NEWS2 ≥ 7 threshold: A high aggregate score should be treated as an independent and powerful trigger for emergency clinical assessment and possible care in a monitored or critical-care environment.
Rapid escalation trajectory: Even if the baseline score is low, a sudden increase of +2 points or more over a short time window suggests dynamic deterioration and may precede cardiopulmonary collapse.
Refractory NEWS2 ≥ 5 state: A medium score that fails to respond to initial interventions such as oxygen titration or fluid bolus requires early escalation and reassessment of the care level.
Universal critical red flags beyond NEWS2
Overt respiratory failure: Worsening arterial blood gases, exhaustion of accessory respiratory muscles, and need for invasive mechanical ventilation or non-invasive support such as NIV, BiPAP, or CPAP.
Hemodynamic shock: Systemic shock that does not respond to large fluid boluses and requires intravenous vasopressor support.
Acute neurological deterioration: Abrupt GCS drop to ≤ 8, sustained focal neurological signs, or refractory status epilepticus.
Catastrophic metabolic derangement: Life-threatening metabolic acidosis, severe electrolyte disturbance such as hyperkalemia, or urgent need for emergency renal replacement therapy.
Additional red flags that should not wait for the score
Rising oxygen requirement: A patient who was on room air and now needs escalating oxygen is deteriorating, even before NEWS2 reaches 7.
New confusion: New delirium is a marker of systemic, respiratory, metabolic, or neurological failure until proven otherwise.
Low blood pressure with poor perfusion: Cold peripheries, delayed capillary refill, oliguria, or raised lactate.
Marked tachypnea: Respiratory rate is often the earliest sign of deterioration and should not be dismissed as anxiety.
Failure of initial therapy: Persistent hypoxemia, hypotension, or confusion after first-line interventions should trigger early escalation.
Management Plan
What the on-call clinician should do when NEWS2 ≥ 5
Go to the patient: Do not manage the score by telephone alone. Perform or directly supervise an ABCDE assessment.
Confirm the observations: Repeat vital signs if they are inconsistent, but do not use repeated measurement as a way to delay escalation.
Start initial treatment: Appropriate oxygen, IV access, fluids when indicated, urgent blood tests, blood gas, lactate, glucose, ECG, cultures and antibiotics when sepsis is suspected, and imaging according to the clinical picture.
Define the level of care: Ward with closer monitoring, HDU, or ICU.
Escalate clearly: Use SBAR when calling for help: state the score, reason for concern, trajectory, what you have done, and what you need now.
When an ICU request becomes clinically convincing
NEWS2 ≥ 7 with clinical deterioration, oxygen requirement, shock, or impaired consciousness.
NEWS2 ≥ 5 that does not improve after initial treatment.
Rapid increase in score over a few hours.
Likely need for NIV, CPAP, BiPAP, intubation, invasive monitoring, vasopressors, or emergency renal replacement therapy.
Serious underlying disease with low physiological reserve, such as severe COPD, advanced heart failure, immunosuppression, or major postoperative status.
Strong clinical concern despite a score that is not yet high: the clinician sees a deterioration pattern the score has not fully captured yet.
Ready-to-use escalation call to critical care or rapid response
“This is Dr. (...) calling from ward (...). I am calling about a (...) year-old patient with a NEWS2 of (...) now, previously (...). The main concern is (...): breathing / blood pressure / consciousness / oxygen requirement. I have already done (...). The patient is not improving / is deteriorating rapidly. I need urgent critical-care or rapid-response assessment now, and I think the patient may need (...).”
Practical rescue point: Do not only say “NEWS2 is seven.” Say why it is seven, how it reached seven, what failed to improve, and what level of intervention you expect the patient may need.
Pearls and Pitfalls
Common on-call traps
The low-score trap: A patient deteriorating rapidly may be dangerous before reaching NEWS2 ≥ 7.
The oxygen-mask trap: Acceptable saturation on high-flow oxygen is not normal. The oxygen requirement itself is a danger signal.
The ignored-respiratory-rate trap: Respiratory rate is one of the most sensitive markers of deterioration, but it is often estimated poorly or ignored.
The confusion trap: New confusion is not “just sleepiness” until proven otherwise. Think hypoxemia, sepsis, shock, glucose disturbance, medication effect, or neurological pathology.
The waiting-for-labs trap: Do not wait for lactate or blood gases if the patient is clinically collapsing.
The score-instead-of-exam trap: NEWS2 does not examine the abdomen, listen to the lungs, see bleeding, or read your bedside concern. Examine the patient.
The late-escalation trap: Calling critical care after everything has failed is worse than calling early when the collapse is beginning.
Practical on-call pearls
If NEWS2 rises, search for the cause, not only the score.
If NEWS2 is ≥ 5, ask: do I need review within an hour? Do I need blood gases? Do I need a higher-level team?
If NEWS2 is ≥ 7, ask: does this patient need continuous monitoring, HDU, or ICU?
If one parameter scores 3, do not be falsely reassured by a low aggregate score.
If consciousness changes or oxygen requirement rises, escalate early.
If treatment improves NEWS2, document the response and the next monitoring plan.
Rapid on-call summary
NEWS2 0-4: low risk, but watch for a single red score or rapid upward trend.
NEWS2 5-6: urgent review, assessment within 60 minutes, and a clear plan.
NEWS2 ≥ 7: immediate response, often involving critical care or rapid response.
NEWS2 does not replace clinical judgement.
Respiratory failure, shock, GCS ≤ 8, refractory seizures, and dangerous hyperkalemia override the score.
Do not treat NEWS2. Treat the patient whose physiology made NEWS2 rise.